






Some of us are old enough to remember when Dr. Anthony Fauci told the nation that “herd immunity” may require 90% of Americans to receive COVID-19 vaccinations. First, that is a complete revision of the meaning of herd immunity since it is not a static concept. Second, while it may have been a legitimate goal to achieve near-zero COVID-19, all it meant was that 90% of the population needed to have an effective immune response to COVID-19. To date, Fauci, the CDC, and the rest of the health agency bureaucrats have defined this response as having detectable circulating antibodies.
If that is the case, why is no one talking about two seroprevalence studies on the CDC website? At a minimum, they raise questions about the public health response, the current pandemic statistics, and the immune response individuals have to a COVID infection after receiving the vaccines. The two studies measure detectable antibodies in the population nationwide.
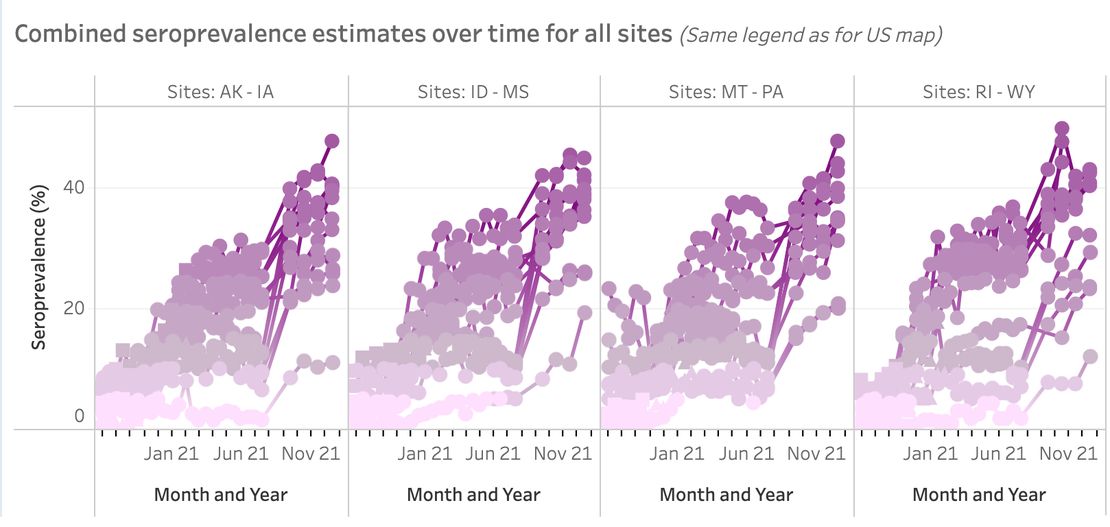
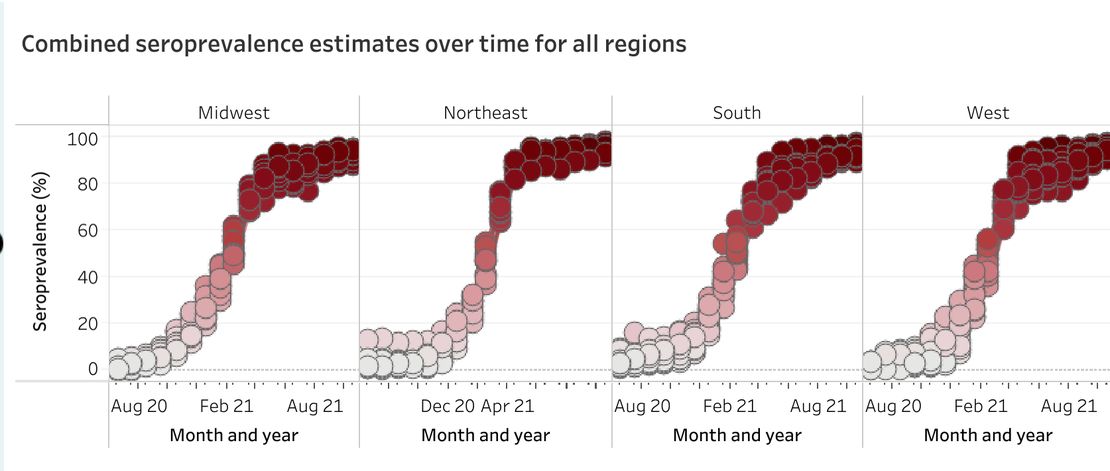
The first is the commercial laboratory study constructed to detect people who have recovered from an infection. To be considered antibody-positive after recovery, a person needed to be positive for N, or nucleocapsid, antibodies as well as the S, or spike protein, antibody. The second is the blood donor study, which looked at people who recovered and those with vaccinated immunity. That study used the presence of the N antibody to differentiate between the recovered and the vaccinated.
According to the commercial lab study, between 33.1% and 34% of the population have circulating antibodies following a COVID infection as of 12/26/2021. For children 17 and under, approximately 44% show evidence of antibodies from prior infection. To emphasize, nearly half of the children under 17 express recovered immunity, and in two years, less than 1,000 have died. Yet Pfizer and Dr. Fauci are talking about giving toddlers and infants three doses of an experimental vaccine. And teachers’ union president Randi Weingarten wants 80% of school-age children to be vaccinated before masks come off.
The interesting part of the analysis is that the levels of immunity are cumulative. Yet the CDC clings to the idea that there is no data to support durable immunity longer than 90 days. Travel to the U.S. requires a negative test within a day of departure or proof of recovery from a confirmed case of COVID in the last 90 days. Yet the estimates for the acquired immunity never decline in the study.
The blood donor study estimates the combined recovered and vaccinated immunity nationwide at almost 94% as of Feb. 8, 2022. Once again, the estimates for immunity in the population never decline.
Yet, the CDC and several studies have shown the effectiveness of vaccinated immunity declines over time. In fact, on Friday, the CDC announced the boosters wane after four months:
Researchers found the booster shots remained highly effective against moderate and severe covid-19 for about two months after a third dose. But their effectiveness declined substantially after four months, suggesting the need for additional boosters, the study said.
The vaccine was 91% effective in preventing a vaccinated person from being hospitalized during the two months after a booster shot, the study found. But after four months, protection fell to 78%.
Protection faded more in preventing trips to urgent care and emergency departments, falling from 87% in the first two months to 66% after four months. After more than five months, vaccine effectiveness fell to roughly 31%, but researchers noted that estimate was “imprecise because few data were available” for that group of people.
The first question is, if seroprevalence is not waning over time, why does the vaccine’s effectiveness? With such high levels of vaccinated and recovered immunity, why are health officials talking about additional boosters? An update from Johns Hopkins’s study of natural immunity demonstrates recovered patients have circulating antibodies to COVID nearly two years after recovering.
This question becomes even more urgent with the highly transmissible Omicron variant. Among the study participants for Johns Hopkins, 11% of participants who reported being COVID naive and unvaccinated displayed S antibodies. On PCR tests, the U.K. used the lack of a reaction to the S protein as a proxy for detecting Omicron rather than Delta. In fact, the lack of response to the S gene on testing was the red flag that caused South African health officials to believe they had a new COVID variant in four foreign travelers.
Have scientists even determined if COVID-naive unvaccinated individuals make S antibodies detectable by current tests following infection with Omicron? Researchers must answer this question to assess seroprevalence accurately. Anecdotal evidence from my own online interactions and conversations in real life indicates a percentage of people far higher than 30% have experienced a COVID infection at this point in time. This assessment is true whether they were vaccinated or not.
The second question is whether the lack of N antibodies really rules out an infection in vaccinated individuals. According to the ZOE COVID study, one in five recovered patients does not have detectable N antibodies. The U.K. Health Security Agency also issued a report in late 2021 that noted that patients who recovered from COVID after receiving two doses of the vaccine developed fewer N antibodies than unvaccinated people that became infected. Vaccinations have been available for over a year, and the CDC reports 80.5% of Americans over five have had at least one dose. How is the CDC sure it is capturing all post-vaccination infections using the current study model?
Finally, if the nation has hit Dr. Fauci’s 90% goal for expressing immunity through recovery or vaccination, why is 98% of the country still considered to have high transmission according to the CDC?
![]()
It is good news the CDC has data on seroprevalence. However, there should be tons of questions about why they are not relying on it to manage the pandemic, make recommendations, and assess overall risk. For example, how does less than 10% of the population drive the transmission, hospitalization, and death numbers the agency and the media are reporting? Especially when many unvaccinated people are under 40 and less likely to suffer severe illness and death?
Also, the agency tells Americans that vaccines prevent severe illness and death. Multiple studies demonstrate recovered immunity also provides that protection. How is it possible we are still in a high-risk situation, according to the CDC’s transmission map? Is more than 100 positive tests per 100,000 residents the right cutoff? And why is the agency even considering percent positive on testing as a metric, with home testing and varying test rates nationwide?
That the seroprevalence data exists and the health bureaucrats never discuss it is disturbing enough. That it has changed nothing about the pandemic response, vaccine program, or agency risk assessment is stunning.
Story cited here.
















